

Artificial Intelligence in Healthcare: A Practical Guide
Artificial intelligence in healthcare is a set of software systems that learn from medical data to help clinicians spot disease earlier, read scans faster, and make better decisions at the point of care. It is not a robot doctor. It is a layer of pattern recognition that sits behind the people who already do the work, and when it is built well, it gives them back time and catches what a tired human eye can miss.
The hype around this field is loud, and most of it skips the hard part. A model that wins a benchmark in a research paper is a very different thing from a system that holds up in a hospital at 3am, where the data is messy, the stakes are real, and a wrong answer is a patient-safety event. This guide cuts through that gap. You will see where artificial intelligence in healthcare is genuinely delivering results today, where it still fails, and the engineering discipline that decides which side of that line a project lands on.
What is artificial intelligence in healthcare?
At its core, this is machine learning applied to clinical problems. You take a large amount of labelled medical data, such as scans, lab results, notes, or vital signs, and you train a model to recognise the patterns that map an input to an outcome. The trained model can then flag a likely diagnosis, predict a risk, or surface the relevant record for a clinician to confirm.
The key word is confirm. In a serious clinical setting, the model does not decide. It proposes, and a qualified human disposes. That single design choice separates a tool doctors trust from one that gets switched off after a month. The most useful systems are quiet assistants, not loud oracles.
It helps to see where these systems actually sit in the flow of care. They are not one big brain. They are many small models, each plugged into a specific moment where a decision happens.

Notice that a clinician sits in the middle of the chain, not at the end of it. Every model feeds a person, and the person stays accountable for the call. That is the shape of healthcare AI that works in practice.
How is AI used in healthcare today?
The field is wider than most people think, because the useful wins are unglamorous. They are not headline cures. They are small reductions in error and delay, repeated across millions of cases. Here are the areas where AI and healthcare already overlap in production.
- Medical imaging. Models read X-rays, CT scans, MRIs, and pathology slides to flag suspicious regions for a radiologist. This is the most mature use of AI in the medical field by a wide margin.
- Early risk prediction. A model watching vital signs and labs can warn that a patient is trending toward sepsis or deterioration hours before it becomes obvious.
- Clinical documentation. Speech models turn a doctor-patient conversation into a structured note, which gives clinicians back the hours they lose to paperwork every day.
- Drug discovery. Models screen huge chemical spaces to predict which compounds are worth testing in the lab, compressing years of trial and error.
- Triage and operations. Risk models help decide who needs to be seen first and how to schedule beds, staff, and theatres without waste.
For example, a sepsis early-warning model does not diagnose anything on its own. It quietly scores every patient on the ward every few minutes and raises a flag when the numbers drift the wrong way. The nurse still checks the patient. The model just makes sure the patient gets checked sooner. That is the whole value, and it is enormous.
AI in medical diagnosis and imaging
Diagnosis is where artificial intelligence in healthcare gets the most attention, and for good reason. Reading a medical image is a pattern-matching task, and pattern matching is exactly what deep learning is good at. An imaging model can be trained on hundreds of thousands of scans, far more than any single radiologist will see in a career.
The practical effect of ai medical diagnosis is not replacement, it is amplification. The model acts as a second reader that never gets tired and never has a bad day. Studies of imaging models have reported error reductions in the range of 5 to 20 percent on specific tasks when a model and a clinician work together, compared with the clinician alone. The gain comes from catching the rare, easy-to-miss case, not from being smarter on the obvious ones.
Here is how a well-built ai diagnosis tool actually fits into the workflow. It does not hand the doctor an answer. It hands them evidence.
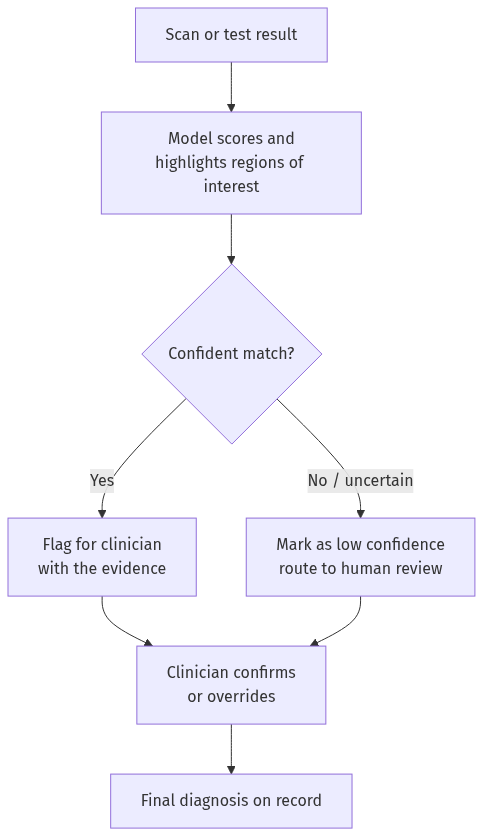
The same pattern holds for artificial intelligence in medical imaging across radiology, pathology, and ophthalmology. The model narrows the search and ranks what to look at first. The specialist makes the call and signs their name to it. When you see a vendor claim a model “diagnoses” anything by itself, treat it as a warning sign, not a feature.
Where AI is actually delivering results
Not every use case is at the same level of maturity. Some are deployed and trusted in hospitals right now. Others are promising demos that fall apart on real data. Being honest about that difference is the most useful thing an engineer can offer. Here is how I rate the main areas by how ready they are for production.
| Use case | Maturity | Why |
|---|---|---|
| Medical imaging triage | Deployed and trusted | Clear inputs, huge labelled datasets, a human always confirms |
| Documentation and notes | Deployed and growing | Saves hours, low clinical risk, easy to verify the output |
| Early deterioration alerts | Deployed, needs tuning | High value, but false alarms cause alert fatigue if poorly built |
| Drug discovery screening | Maturing fast | Speeds up research, but lab validation is still the real test |
| Autonomous diagnosis | Not ready | No safe path to remove the clinician from the loop yet |
The pattern in that table is consistent. AI succeeds where the input is well defined, the data is plentiful, and a human verifies the output. It struggles where any of those three is missing. If you are deciding where to invest in AI and healthcare, start at the top of that list, not the bottom.
Why adoption is accelerating now
Three forces are pushing artificial intelligence in healthcare from pilot projects into daily use, and they are worth understanding because they shape where the field goes next.
The first is data. Hospitals have spent the last decade moving to electronic records, which means the raw material for training models finally exists at scale. According to multiple industry surveys, a majority of health systems now run or pilot at least one AI tool, up sharply from a few years ago. The second force is staffing pressure. Clinician burnout and shortages are real, and any tool that gives a doctor back an hour a day pays for itself quickly. The third is regulatory progress, as approval pathways for software that informs clinical decisions have matured, so vendors finally have a clear route to market.
The trajectory is steep. Research and market analysts project the healthcare AI market to grow several times over by 2030, driven mostly by imaging and clinical workflow tools rather than the science-fiction use cases that get headlines. For instance, the unglamorous documentation assistant, the one that just writes the note, is spreading faster than any diagnostic model, because the risk is low and the time saved is obvious on day one.
What this means in practice is that the question for most health systems is no longer whether to adopt AI, but where to start and how to do it without getting burned. That is exactly where good engineering judgement earns its keep, because the easiest tool to buy is rarely the safest one to deploy. Picking the right first project matters more than picking the cleverest model.
What still goes wrong with AI in healthcare
I would be misleading you if I made this sound solved. It is not. The failures in artificial intelligence in healthcare are specific, repeatable, and avoidable only if you design for them from the start. Here are the ones I watch for on every project.
Biased training data. A model only knows the patients it was trained on. If that data skews toward one group, the model performs worse on everyone else, and it does so silently. A skin-cancer model trained mostly on light skin will miss cancers on dark skin. The model is not malicious. The data was incomplete, and the model faithfully learned the gap.
Distribution shift. A model trained at one hospital can quietly fail at another with different equipment, different patient mix, or a different scanner. The accuracy that looked great in the paper does not transfer, and nobody notices until outcomes slip.
Confident wrong answers. This is especially true for the new wave of large language models entering clinical tools. A model will state a fabricated drug interaction in the same calm tone it uses for a correct one. In a field where a confident wrong answer is a liability, that tone is the danger, not just the error. I wrote a full breakdown of why LLMs hallucinate and how to keep them grounded that applies directly here.
Automation bias. When a tool is usually right, humans stop checking it. The danger is the rare case where the model is wrong and the tired clinician agrees on autopilot. Good design fights this by showing evidence, not just an answer, so the human stays engaged.
None of these mean the field is a dead end. They mean the engineering is the product. The model is the easy part. The system that catches the model when it fails is the hard part, and it is what separates a safe tool from a risky one.
How to build AI for healthcare safely
Building artificial intelligence in healthcare that is safe to ship is less about model architecture and more about discipline around the model. The work I trust follows the same stack every time, and each layer exists to catch a failure the last one missed.
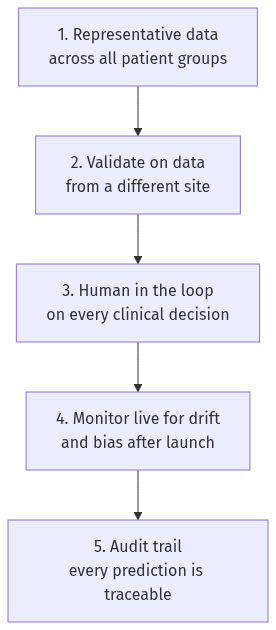
Let me walk through why each layer earns its place.
Representative data. Before any modelling, you check that the training data covers the patients the system will actually serve, across age, sex, ethnicity, and equipment. If a group is missing, you fix the data, not the model.
External validation. You test the model on data from a site it never saw in training. A model that only works on its home data is not a product, it is a lab result. This single step kills most over-optimistic projects, and that is a good thing.
Human in the loop. For any decision that affects a patient, a qualified person confirms the output. The model proposes evidence, the clinician decides. This is not a temporary safeguard. In high-stakes care, it is the permanent design.
Live monitoring. Once deployed, you watch the model the way you watch a patient. Accuracy drifts as the world changes, so you track it continuously and retrain before performance slips, not after.
Audit trail. Every prediction is logged with the data it saw and the version that produced it. When something goes wrong, and eventually something will, you can trace exactly what happened and fix it.
That stack is unglamorous, and that is the point. The teams that ship healthcare AI safely are the ones that treat the boring layers as the real engineering. I learned this building a patient diagnostic system, where the model was maybe a fifth of the work and the validation and safety scaffolding around it was the rest.
Frequently asked questions
How is AI used in healthcare?
AI is used in healthcare mainly to support clinicians rather than replace them. The biggest areas are medical imaging, where models flag suspicious findings on scans, early risk prediction that warns of patient deterioration, clinical note-taking, and drug discovery. In every mature use, a qualified human confirms the output before it affects a patient.
Is AI safe in healthcare?
AI can be safe in healthcare when it is built with the right safeguards, and risky when it is not. Safety comes from representative training data, validation on outside data, a human confirming every clinical decision, and live monitoring for drift and bias. The model itself is not the safety feature. The system around it is.
Will AI replace doctors?
No, AI will not replace doctors. It changes what doctors spend their time on by handling pattern-heavy tasks like first-pass scan reading and paperwork. The clinical judgement, the accountability, and the human relationship stay with the doctor. The realistic future is a clinician working with AI who outperforms one working without it.
What is the biggest risk of AI in the medical field?
The biggest risk is a confident wrong answer that a busy clinician accepts without checking. This is made worse by biased data, which causes silent failures on under-represented patient groups, and by automation bias, where humans stop verifying a tool that is usually right. Good design surfaces evidence and uncertainty so the human stays in control.
The takeaway
Artificial intelligence in healthcare is not a future promise. It is already reading scans, warning of deterioration, and writing notes in hospitals today. But the value is never in the model alone. It is in the careful system that grounds the model in good data, validates it honestly, keeps a clinician in the loop, and watches it after launch.
If you remember one thing, make it this. In healthcare, the model is the easy 20 percent and the safety engineering is the hard 80 percent. The teams that respect that ratio build tools clinicians trust. The ones that chase the benchmark and skip the scaffolding build demos that quietly get switched off. If you are working on a healthcare AI project and want to talk through the architecture, reach me on LinkedIn or through the contact page.
About the author
Ayaz Qaiser is a senior AI engineer with eight years of experience building machine learning and LLM systems in healthcare and finance, where a confident wrong answer is a real liability. He has shipped a patient diagnostic platform and production clinical tools, and writes about how AI actually behaves once it leaves the demo and meets real patients.